Diabetes in Pregnancy
The mainstay of the medical management of diabetes involves frequent monitoring of blood glucose levels with adjustment of diet and insulin therapy to achieve normoglycemia.

The mainstay of the medical management of diabetes involves frequent monitoring of blood glucose levels with adjustment of diet and insulin therapy to achieve normoglycemia. Normoglycemia is important because maintenance of maternal blood glucose concentration at or near normoglycemic levels decreases the likelihood of adverse pregnancy outcomes, such as miscarriage, congenital anomalies, macrosomia, and fetal death. Ideally, normoglycemia is achieved before conception and maintained through the postpartum period. The ADA recommends a pre-conception A1C goal of <6.0 percent.
Blood glucose monitoring can vary with the severity of the diabetes. At a minimum, diet controlled gestational diabetes requires four values, one fasting blood sugar (fbs), and three one hr postprandial after breakfast, lunch, and dinner. Patients with more advanced diabetes who are on short acting insulin, varying eating schedules, and the insulin pump, can also add pre-prandial and middle of the night values. Standard goals are fbs 60-90, 1hpp < 140, 2hpp < 120, mean capillary glucose 100, A1C < 6.0, night glucose levels no lower than 60.
Patients should be referred to our diabetic counselor for appropriate diet management. If she cannot meet the goals set above on diet alone, then either glyburide or insulin can be started. Most gestational diabetics in which the diagnosis is made in the third trimester do well with glyburide. Glyburide can be given as 2.5 mg po qam and, if needed, 2.5 mg po qhs, and increased by 2.5 mg po until the maximum dose of 10 mg po qam and 10 mg po qhs is achieved. (20 mg po total daily dose). If glyburide is not enough to maintain the glycemic control goals, then insulin can be started.
The insulin pump is becoming more popular because it involves one stick every three days and a great amount of flexibility. In addition, we also have the continuous glucose monitoring probe. This combination offers the greatest flexibility and accuracy in treating insulin dependent diabetics.
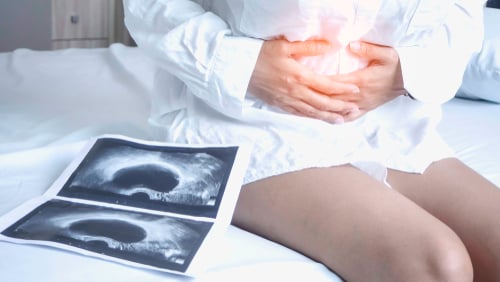
Serial ultrasounds will be needed to monitor growth. Genetic screening and possibly invasive testing may be needed. Detailed anatomy scan should be performed. For pre-gestational diabetics, a fetal echo is indicated. Antenatal testing should occur at a minimum weekly starting at 32-34 wks. Delivery in diet controlled can occur after 39 wks but patients on glyburide and insulin should be delivered at 39 wks.
Diabetes is a common and potentially serious problem during pregnancy. Our practice has extensive experience in treating diabetes in pregnancy. We run the entire gamut from diabetic educators, Maternal and Fetal Medicine specialist, and Obstetricians. Our practice is an expert in using diet, oral hypoglycemic, insulin, and insulin pumps in the management of diabetes in pregnancy. Our expertise in ultrasound extends to all aspects of Obstetrical imaging including fetal echocardiograms. We use a multifaceted team approach to the management of diabetes in pregnancy and have excellent outcomes. We have extensive resources, experience, and expertise in managing these complicated patients.